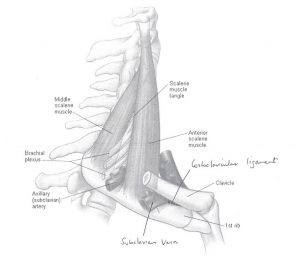
The brachial plexus and subclavian artery course through a triangle as they make their way to the arm. The triangle is bounded by scalenus anterior and scalenus medius at the front and back with the first rib as the base.
Nerve symptoms or arterial compression are caused by the space being reduced especially during elevation and external rotation of the arm, such as movements made when brushing your hair or when hanging washing on the clothesline.
If these symptoms become troublesome, the first step is physiotherapy by an experienced practitioner in this area. If exercises and strengthening programs fail after an extended trial of treatment, consideration may be given to decompression of the thoracic outlet by surgical means.